We've now reached the point where the stuff you can buy over the
counter is stronger than anything you can buy on the street.
- Denis Leary
THE D X M ZINE.
Issue 12. July 2002.
A Symposium of Articles Pertaining to DXM Use
(c)2002 Jeffrey Sothen/gravol
Email at [email protected]
Official Zine Web Site at http://www.dextroverse.org/~zine
Official Zine Web Site Mirror at http://www.third-plateau.org/dxmzine
RFG's Zine Web Site Mirror at http://www.dextromethorphan.ws/zines
Edited by gravol, with article contributions by fellow DXMers.
DISCLAIMER
: The authors of this zine do not condone the use of dextromethorphan
in any way. This text is simply used as an informative guide to issues
relating to dextromethorphan use and should be used for entertainment
purposes only. We are not responsible for any actions taken by anyone
reading this text.
WARNING
: While the authors of this zine do not condone the use of
dextromethorphan in any way, a strict warning also is warranted here
regarding the dangers of Coricidin Cough & Cold. Each year, the rate
of death of individuals who overdose from this dangerous medication
increases, and for this reason this zine will no longer publish trip
reports involving this medication, nor will we publish any information
that may cast Coricidin Cough & Cold in a positive light. Anyone
still using this medication should stop immediately, because of the
dangers of the secondary active ingredient, chlorpheniramine maleate.
---
CONTENTS
1 From the Editor
2 Announcements
3 Letters to the Editor
4 DXM in the Media
5 The First DXM Street Gang
6 Old Man Dies of DXM Overdose
7 New DXM/Morphine Product a Flop
8 DXM Medical Breakthrough?
9 The Lasting Effects of DXM
10 The DXM Birth-Defect Scare
11 A DXM Nightmare
12 A Brief Synopsis of DXM as a Dissociative
13 DXM and Dream Research
14 The DXM Enigma - The Pyramids and 11:11
15 The How's and Why's of CEV's
16 An In-Depth Look at DXM Abuse
17 Tales from the Darkside
18 DXM Artwork
19 Info on Ordering Pure DXM Powder
20 Acknowledgements/Zine Information
---
FROM THE EDITOR
Greetings,
You have quite an issue in front of you so I will make this as short
as possible. I just want again draw attention to the new format of the
Zine. From now on, it will be in this format (RTF). If you have any
questions or comments, please be sure to contact me.
There is quite a bit of news in the Announcements
section, so please do not pass that up either. We will be starting up
polling soon and that is why it is important that you subscribe to the
DXM Mailing List if you haven't already done so, otherwise you won't be
in the drawing for free DXM powder.
Other than that, be safe and enjoy your summer!
gravol
St
Augustine, FL
June
27, 2002
ANNOUNCEMENTS
THE DXM RESEARCH PROJECT AND OTHER ANNOUNCEMENTS
compiled by gravol
DXM Research Project:
The DXM Research Project is still in its beginning stages. So far,
Vaesolis from the Dextroverse has been able to raise over $4000, but the
project is very slow to take birth - so please be very patient, and we
will update you with any new information. Also look for a future
interview with Dr. J.M. Olney by Vaesolis. If you have any comments or
questions regarding his project you can contact him at:


[email protected]
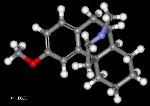
Dr.
J. M. Olney
A
DXM molecule
Courtesy of Erowid
NEW FORMAT FOR THE ZINE
by gravol
The Zine is upgrading to a more graphic-friendly environment. We will
now distribute the Zine in RTF (Rich Text Format), which can be viewed
with MS Word or WordPad (WordPad comes already installed with your
computer). You should not experience any problems in viewing this new
format, but if you do, you can contact me at [email protected].
This new format will allow a better viewing capacity for
the reader, along with the implementation of graphics. All new issues
will now appear in this new format. We are interested in getting your
feedback regarding these changes, so feel free to contact me and let me
know how you feel about the changes, or how we can better accomodate
you!
We have also scaled back some sections of the Zine in this
issue because of size limitations. I was not aware of how much file
space RTF files took up, but rest assured you can find these sections
(DXM Poetry and Music/Movie Reviews) in future editions.
DXM PREPS UPDATED, NOW IN SEPARATE FILE
by gravol
The list of DXM-containing preparations has now been updated to
include all OTC medications containing DXM in Australia, and because of
the size of this list, these preparations will now be listed in a
separate file which will be available with the Zine each time it is
distributed. The filename, PREPS.TXT, will remain the same until it is
updated further.
NEW DXM CONTEST AND FREE DXM GIVEAWAYS!!!
by Staff
The DXM Zine will now be giving away free DXM HBr in powder form
exclusively to contributors of the Zine. All articles must be submitted
by the 20th of each month, and one entry per email person will be
submitted for a monthly drawing. The approximate amount that will be
given away will be 10 grams each month. Special thanks to the
Dextroverse for help making this possible. If you would like a chance to
win free DXM then please contribute and make yourself known to the DXM
community!
Upon receiving an article contribution, you will receive
notification that you've been entered in the contest and the winners
will be announced in each upcoming Zine. Good luck!
NEW SECTION ANNOUNCED - TALES FROM THE DARKSIDE
by gravol
DXM is a drug shrouded in mystery. And as DXM use grows more bizarre,
so does the drug's users. This new monthly section highlights the
bizarre behavior of a selected few individuals who use DXM and act
rather strangely on it - read the section, you'll know what I mean!
Another warning must be given here in that we do not condone any of the
behavior of such individuals, but would like to cast some light onto
some of the odd and bizarre things that are going on out in DXM-land
that we feel the readers should know.
RFG ANNOUNCES ZINE UPDATE FOR HIS WEBSITE
by gravol
Robert F. Golaszewski, who is well-known for promoting the dangers of
Coricidin, has starting publishing back issues of the DXM Zine in HTML
format at his website, http://www.dextromethorphan.ws and will only contain issues 1-10, with current issues being available at the Dextroverse at http://dex.kenton.org/dxmzine
'DXM IN THE MEDIA' SECTION REVISED
by gravol
Due to complaints from subscribers, I have revised this section to
include only brief excerpts from recent news articles instead of
full-length stories. However, any news regarding DXM deaths will be
fully reported to the best of my ability.
LETTERS TO THE EDITOR
From: [email protected]
Great zine, still reading through it. Of course, the section on
11:11 freaked me out.... Here's an email I sent my friend Tim in late
1999:
crazy
stuff. i'm off dxm for good, did my last trip last night (4th
plateau) and had a very strong metaphysical conversation with the powers
that be. Still, the price on my body is too high.
the 11:11 stuff had been happening for quite some
time after I started DXM. I would look down at my watch, and it
was always 11:11. So i
wondered if it was a function of the 'real' global time or perhaps
just the local time on my watch or my computer. nonetheless, it
didn't matter, i always ended up seeing 11:11.
I would be at work and glance down at my watch and see it
at 11:11, or perhaps be with my friends and ask what time it was, and
it would be
11:11. as for the dxm stuff, I'm done it way too many times and
need to stay off it, as i think I've gotten all I can from it. It
started as a curious fascination with the hallucinations and extended to
the metaphysical as I got deeper and deeper into it. During my
higher plateau trips, I cannot help but feel that I am creating my own
time-line reel and am witnessing creation itself, but in a strange way.
These last few trips, I nearly passed to the other side, with my body's
defense mechanisms kicking in to 'save me'. It could have been the
trip, but I think it's also dxm's toll on the body. no more.
Btw, just finished reading your section on CEV.... Simply
mindblowing...I've never read anyone else's description quite as
accurately as this.
I've been fascinated by many of these same questions since I started
DXM'ing in late 1998, and have been keeping a very detailed journal of
my experiences
these last few years, particularly on the imagery. I am currently doing
research at UIUC (starting this fall), the Beckman Institute (http://www.beckman.uiuc.edu), and hopefully will get to do some research of the type you proposed in your zine.
DXM IN THE MEDIA
 DXM ON TELEVISION
DXM ON TELEVISION
compiled by gravol, Vaesolis
It came to my attention that there has been recent references to DXM
abuse on national and local television. For instance, on Everybody Loves Raymond
, Raymond and his brother apparently popped a large quantity of
Sucrets to get high, and this led to a comedic scene once Raymond's
parents came home and discovered them acting strangely.
There has also been recent reports of DXM abuse mentioned
on Montel Williams in a much darker tone, namely Coricidin, and on
several local news stations exposing the dangers of Coricidin. It is
very rare for any mention of DXM to come up that mentions it in the
syrup form or the powder form.
DXM IN THE NEWSPAPERS
compiled by gravol, rfgdxm, void
In Carroll County, MD, Times staff writer Mia Burns quoted Mark Yount,
a substance abuse coordinator, as saying "This is brand new to Carroll.
We have young clients coming in
with use of Coricidin, probably 15-, 16- and 17-year-olds. That's what we're seeing around the country."
In San Antonio, TX, Cindy Tumiel of the San Antonio Express-News
reports to us that "A teen brought over-the-counter cold medication to a
local psychiatric outpatient program and shared it with three other
students on Monday, resulting in all four being sent to hospitals,
officials said." That medication turned out to be Coricidin Cough &
Cold, which again highlights the dangers of this deadly medication.
In Central Ohio, Misti Crane, a Dispatch medical writer, noted that
"Last year, the Central Ohio Poison Control Center had 41 calls about
Coricidin," and Mohamad Moinzadeh, a counselor who works with adolescent
drug and alcohol abusers at University Hospitals East's Talbot Hall,
estimates that 30 percent of teens have abused the medication.
In Utica, NY, staff writer Jon Ottman reports about a Matt Davis, 17,
who died of Coricidin intoxication in January and a high level of abuse
at local highschools.
In Greenwich, CT, Nadia Lerner reports a surge in Coricidin abuse at local highschools.
THE FIRST DXM STREET GANG

INDIANA GANG ROAMS ABOUT, BREAKING THE LAW AND STEALING CORICIDIN
Exclusive by gravol
I recently received a letter from a DXM user who claims to be part of a
street gang in Elwood, Indiana. This is the first time I have heard of
an actual "gang" involved DXM abuse. The gang, Coricidin Soldiers,
is described in more detail in this email I received from one of its
members:
The
initiation rights are first you must be presented to the group by
another member. So, if you wanted to be in you would have to get a
member to vote you in. Then we take a vote with all the members.
If you win the vote than you do a little initiation where it go's
1) steal robo-max from CVS, 2) collect ingrediants to extract Dex. 3)
Succesfuly make Extracted Dex. 4) Down robo. 5) Reach 4th Plateau and
spend whole 4th plateau trip in a completely black closet. You
must do the initiation with a leader present. We're thinking up
more initiations right now but we've done this a few times and it's
worked so far. We sometimes use Coricidin but for the most part is
dex. Myself personally have used it to meditate sometimes but for
the most part it's just getting all the members, going out to the club,
getting dexed out and passing out some time around 5:00 am.
Coricidin soldiers began when Tim and his brother Keven learned
about it. They started doing it, some others started doing it, and
then they just decided to start a group of people who do it. I
don't know how they learned about Coricidin, I cant get a hold of them.
They were put in jail but I learned about it from my cousin.
Then I looked at your website and found out about robo and my
cousin and I started our own club. There's about 10 members, 3
taking the initiation right now, and us 3 leaders.
We don't really have a gang history yet since we just
started the group but there was this really funny story with us were we
had all brought LOTS and LOTS of cans of spray paint and we were going
to spray paint the club and I guess we closed the windows and doors
because after about an hour and our robo-buzz had kicked in we all
started seeing shit really bad (worse than just regular robo) and we
were all light headed. Than we realized that we had the
ventilation (doors and windows) all shut and the fumes from the paint
were fucking us up. Also another one was when we broke into a
hardware store to steal lots of helium and take it out to the club.
Turns out we stole nitrus oxide. The pure shit. You
can imagine how fucked up we got.
There a few people in our town that dex. Probably
about 50-100. Most are teens but some are adults.
You can reach this individual at [email protected] if you have any questions.
OLD MAN DIES OF DXM OVERDOSE
 THE STRANGE TALE OF HERBERT JOHNSON, WHICH TURNED OUT TO BE A HOAX OF GRAND PROPORTIONS
THE STRANGE TALE OF HERBERT JOHNSON, WHICH TURNED OUT TO BE A HOAX OF GRAND PROPORTIONS
Exclusive by gravol
On April 20, a strange event unfolded on Usenet's
alt.drugs.psychedelics. The case involved a senior citizen who
reportedly had too much cough syrup to drink:
"I am 72 and distraught over losig most f my stck in enron and my dog
howsr so i followd yor advicd n got 2 8oz bottls of tussin flu (usded to
have morphne back in my day0 and alredy drank one an an njow im strting
to see the walls thyr shiny smooth like alien membran ohhh
what am i doin stupid old man can any of you help me. grandson got me
conput for bdya and ben foolin round wwit it and been deprssed so i drnk
yor shit i DRANK it, you boys dont kno good nrcs if thd hit u n tha
face but oh ohh man gttn hrd to seetype, im goinimgoin to lay down
keeeep sseing eys wtchng me mim scrared daa.//a"
Well, you may think this is just another rambling of a dexer, but what
followed was even stranger. His alleged wife posted a followup message
faulting blame at the newsgroup after finding him slumped over, and then
3 months later this news story surfaced from one of my subscribers:
PRESCOTT VALLEY, AZ (AP) - A Chino Valley senior citizen has died from
complications resulting from a recreational drug overdose, according to
family attorney Wilford Hancock.
Herbert Johnson, 72, supposedly became distraught after
losing a family pet and consumed three bottles of an over-the-counter
cough medication commonly found in Robitussin products. The death was
primarily ruled a suicide until the family got Hancock involved and
investigated the death further.
It was then found that Johnson, a retired electrical
engineer, had gotten the information off an Internet site that promoted
the recreational use of the drug, dextromethorphan, as a cure for
depression.
Yavapai County assistant medical examiner Emily Padre has
listed the death now as an accident and listed the cause of death as
complications resulting from the consumption of dextromethorphan. It is
not clear if any other active ingredients or complications thereof may
have caused the death, or if Johnson was currently taking prescription
medication.
His wife told police that when he was initially discovered,
he was face-down at his computer desk with the computer screen on. On
the screen was apparently instructions from several Internet users on
how to abuse dextromethorphan-containing products. A check by local
police found that the Internet site was a message board accessible to
anyone with a modem and Internet connection. The DEA and FBI were then
contacted pending an investigation.
Hancock believes that appropriate action will be taken
against those who passed the information along to Johnson. The entire
Internet site is also currently under close scrutiny by the federal
government, since state and local government agencies have no
jurisdiction over that site, Hancock said.
After being rushed to a county hospital, Johnson was listed in critical condition, where he later died.
His son, Henry, is still very distraught over his
father's death and vows justice will be served against those who coerced
Johnson into taking the medication.
According to Prescott Valley Memorial Hospital,
dextromethorphan abuse has seen a sharp rise over the past two years.
More commonly available in a popular cough-and-cold medication, it can
cause severe hallucinations and suicidal behavior.
Two years ago one man apparently became so distraught
after taking dextromethorphan that he jumped into the Agua Fria River.
Two other teens have apparently hung themselves after ingesting large
amounts of the drug and one toddler had to be airlifted to Good
Samaritan Regional Medical Center in Phoenix after an accidental
ingestion of a dextromethorphan tablet purchased from a rave party.
The Samaritan Regional Poison Center has listed 369
emergency room visits last year from overdoses resulting from
over-the-counter drug abuse and approximately seventy percent are
attributed to dextromethorphan.
According to Jack Reed of the Poison Center the drug is a
chemical that is in the same family as MDMA, which is sold at raves in
Phoenix as "ecstasy." In high doses it can cause homicidal or suicidal
tendencies, self-mutilation, and other erratic behavior. The effects are
similar to mescaline and amphetamine, with symptoms of overdose ranging
from assaultiveness, bowel problems, blackened or discolored tongue,
drooling, dizziness, hallucinations, pallor, panic state, stupor,
tremors, and brain hemorrhage.
A statewide alert has since been issued warning
pharmacies to place the products behind the shelf and permitting only
adults to purchase it.
But even this isn't enough, according to Henry.
"They need to boycott this product and prosecute those
involved with trying to spread it around on the [Internet]. I lost my
father because of it and I'm going on a personal crusade to go after
them. They're in the same boat as terrorists and drug traffickers, and
they're gonna pay for it."
The story was investigated by Trip Magazine, who talked to every
Herbert Johnson in Arizona to try to verify the story. Trip Mag also
tried to contact the misinformed "Jack Reed" to no avail, and discovered
that no other people in the report existed. All in all, it was pretty
humurous in the least - and a valuable lesson to those who either don't
take the time to check the syrup they're drinking or the news story
they're reading.
NEW DXM/MORPHINE PRODUCT A FLOP
ENDO PHARM STOCK TAKES A PLUNGE AFTER NEW DXM/MORPHINE PILL DOESN'T GO OVER WELL
from Dow Jones & Company, Inc.
CHADDS FORD, Pa. -- Shares of Endo Pharmaceuticals Holdings Inc.
(ENDP) slumped Monday after the company said late-stage test results
from its morphine drug combination MorphiDex were "disappointing."
The company said Phase III clinical trials for MorphiDex
showed no statistically significant difference between the trial and
control drugs. Endo said the primary goal of the study was to
demonstrate that the average daily dose of morphine needed for pain
control when given in combination with receptor antagonist
dextromethorphan is less than the dose needed with morphine alone.
Endo said it will continue to analyze the results as it awaits the outcome of two other Phase III trials.
Endo said it recently completed enrollment for the second
of its Phase III trials of MorphiDex, and the company expects the third
of the trials to be completed in the "next couple of weeks." Endo said
it plans to release the results of those studies in the fourth quarter.
Until the company reviews the data from these studies, it
will not be able to resubmit an amendment to the MorphiDex new drug
application with the Food and Drug Administration.
The first Phase III trial of MorphiDex involved 193 chronic pain patients from 20 centers in the U.S.
Shares of Endo Pharmaceuticals were down $4.87, or 46%,
to $5.69 at 4 p.m. EDT Monday on the Nasdaq Stock Market. Earlier in
trading, the stock fell to a 52-week low of $4.98.
DXM MEDICAL BREAKTHROUGH?

NEW DRUG, AVP-923, IS A NEW FORMULATION OF DXM FOR CNS DISORDER PATIENTS
from PR Newswire
SAN DIEGO, -- AVANIR Pharmaceuticals (AMEX:AVN), today announced
completion of a license agreement for exclusive worldwide rights to a
proprietary drug product for the treatment of multiple central nervous
system disorders including emotional lability, neuropathic pain and
chronic cough. The product was licensed from Irisys Research and
Development, a private San Diego contract research organization. An
Investigational New Drug (IND) application for the licensed product, a
new formulation of dextromethorphan internally designated AVP-923, has
been accepted by the U.S. Food and Drug Administration (FDA). Upcoming
Phase II/III studies will assess the drug's efficacy in reducing the
loss of emotional control, clinically known as emotional lability, in
patients with neurodegenerative diseases such as Multiple Sclerosis
(MS), Lou Gehrig's disease (ALS), Alzheimer's Disease (AD) and stroke.
Assuming successful initiation of Phase II/III clinical trials for
emotional lability, the company plans to initiate product development
for the additional indications, neuropathic pain and chronic cough. If
all three indications are successfully developed and marketed by the
company, the addressable market would be in excess of $1.5 billion. "The
license agreement is attractive to us because of the unmet therapeutic
needs, market potential and the fact that there are no upfront payments
by AVANIR," stated J. David Hansen, Vice President of Commercial
Development. "Milestone payments would be made only upon FDA's
acceptance of the filing of an NDA and for FDA marketing approvals for
each indication. If we are successful in obtaining FDA approval and
market the drug, we would pay a royalty based on product sales." AVANIR
is obligated to use commercially reasonable efforts to develop and
commercialize two potential indications for AVP-923, including funding
of all development costs. The company expects that no cash milestone
payment would be paid before 2002, which should provide for more AVANIR
resources to be focused on funding AVP-923 product development. "AVP-923
provides AVANIR with the opportunity to develop the same or similar
formulations for multiple indications allowing us to spread our
development costs and risk across the multiple indications," said Mr.
Hansen. "If we are successful in our strategy, we intend to build our
own marketing and sales organization to sell these products to the
specialty physician markets that diagnose and treat patients with
emotional lability, neuropathic pain, or chronic cough."
AVP-923 is comprised of dextromethorphan and an enzyme inhibitor that
significantly slows the metabolism of dextromethorphan. Currently, the
therapeutic utility of dextromethorphan is limited due to its rapid
metabolism.
Phase I/II clinical trials have demonstrated that AVP-923 provides
sustained therapeutic levels of dextromethorphan utilizing a dose
already familiar to physicians. In neurodegenerative disorders, one of
the symptoms frequently experienced by the patient can be loss of
emotional control. Although not physically harmful, the condition has a
significant affect on the psychological health of both patients and
their caregivers. Medical reports on the incidence of emotional lability
estimate that up to 50% of ALS patients and 25% of MS and AD patients
are affected by the loss of emotional control. In stroke patients the
incidence is initially 20% within the first year of stroke with one-half
of those patients recovering emotional control within the first year.
Currently, there is no FDA-approved product for treating emotional
lability. The FDA has indicated that if the company successfully
performs clinical studies for emotional lability in at least two of the
neurodegenerative diseases, a broad general indication for emotional
lability could be obtained. Combined affected patient populations from
all four diseases result in a patient pool up to 1,000,000 patients per
year. Dextromethorphan is a well known NMDA receptor antagonist and has
been shown to reduce neuropathic pain such as that associated with
diabetic neuropathy. The medical literature indicates that there are
approximately seven million diabetics who suffer from diabetic
neuropathy, 40% of whom suffer from moderate to severe disease. The
company estimates the treatable patient pool is 1,000,000 people.
Currently, the company knows of only one other non-narcotic product
widely in use for treating the chronic pain associated with diabetic
neuropathy, Warner-Lambert's anticonvulsant, Neurontin(R), which has
sales over $800 million annually. Dextromethorphan is well established
as an effective and widely used non-narcotic cough suppressant that is
effective for short periods after each dose. The company believes
AVP-923 could find wide utility for the treatment of chronic cough
typically caused by smoking, post-nasal drip, asthma, gastro esophageal
reflux and chronic bronchitis, as well as intractable cough which is
typically associated with lung cancer. While it is estimated that 11% of
the approximate 30 million physician office visits each year involve
the treatment of cough, the company estimates the treatable patient pool
for chronic and intractable cough indication is much narrower, but
still could be as high as 500,000 patients. AVANIR Pharmaceuticals, a
specialty pharmaceutical company, develops novel therapeutic products
for the treatment of chronic diseases including docosanol 10% cream
recently approved for marketing by the FDA. The company's product
development pipeline includes a patented fully human monoclonal antibody
technology under commercial development. Other programs include a drug
discovery program in the advanced pre-clinical stage of development for
the treatment of the underlying biological causes of allergy and asthma
and preclinical work on novel approaches to discovering compounds with
lipid lowering and anti-inflammatory activities. The information
contained in this press release, including any forward looking
statements contained herein, should be reviewed in conjunction with the
company's Annual Report on Form 10-K and other publicly available
information regarding the company, copies of which are available from
the company upon request. Such publicly available information sets forth
many risks and uncertainties related to the company's business and such
statements, including risks and uncertainties related to drug
development and clinical trials. Preliminary research findings are not
always supportable by evidence obtained from subsequent clinical trials.
Final review decisions made by the FDA and other regulatory agencies
concerning clinical trial results for AVP- 923 are unpredictable and
outside of the influence and/or control of the company. Contact: Patrice
Saxon of AVANIR Pharmaceuticals, 858-410-2660; or Bob Stone, or Ken
DiPaola, both of The Dilenschneider Group, financial media relations,
212-922-0900.
LATE-BREAKING POSITIVE RESULTS REPORTED FOR AVP-923
from PR Newswire
On June 20, 2002, Avanir Pharmaceuticals in San Diego, California
announced positive results from a Phase II/III clinical trial that
tested the safety and effectiveness of Neurodex. The indication for
Neurodex in this study of patients with ALS was pseudobulbar affect or
emotional lability (exaggerated laughing or crying). Avanir reports
that, in this study, the patients in the group receiving Neurodex showed
a greater decline on a rating scale for pseudobulbar affect than those
in two control arms, indicating greater improvement in their
pseudobulbar affect.
Some people with ALS experience symptoms of pseudobulbar affect
including uncontrolled laughing and/or crying in excess of the situation
that prompts the laughing or crying. For many patients and their
families, these symptoms are distressing and can sometimes be
embarrassing. There are no medications indicated to treat pseudobulbar
affect; however, some antidepressant medications are prescribed by
physicians to treat pseudobulbar affect.
Neurodex is a combination of dextromethorphan and an
enzyme inhibitor that allows for "sustained, elevated levels of
dextromethorphan in the body." It is not approved for use by the U.S.
Food and Drug Administration (FDA) at this time. Avanir plans to begin a
second clinical study of Neurodex in pseudobulbar affect in patients
with multiple sclerosis this year. If the results of the MS trial are
positive, the company plans to present its findings and file a new drug
application with the FDA as early as Spring 2004. The FDA requires
positive, adequate and well-controlled studies of Neurodex before the
drug can be approved for general use for emotional lability.
Avanir also plans to initiate an open label trial of Neurodex in
pseudobulbar affect later this year in select locations. This will be an
opportunity for some people with ALS who experience emotional lability
to receive Neurodex and allow for further clinical evaluation of the
safety of this drug over time.
For more information about ALS and pseudobulbar affect, contact The ALS Association toll-free at (800) 782-4747, [email protected] or on ALSA's web site http://www.alsa.org
. For more information about treatments for pseudobulbar affect,
contact your ALS neurologist or health care provider. For more
information about Neurodex or the open label trial of the drug, contact
Avanir Pharmaceuticals at (858) 622-5200 or visit the web site at http://www.avanir.com or contact Mary Lyon, RN, MN, Vice President of Patient Services at [email protected].
Background
Pseudobulbar affect is a condition characterized by frequent episodes
of uncontrolled laughing or crying that do not match a patient's
underlying emotion. It is also known by other terms such as emotional
lability or pathological laughing and crying. Pseudobulbar affect is a
condition associated with a number of neurological disorders, including
ALS.
AVP-923 is a combination of Dextromethorphan Hydrobromide
and Quinidine Sulfate. Dextromethorphan Hydrobromide is a drug that is
available without prescription as an over-the-counter cough suppressant.
Quinidine is one of the oldest prescription drugs still in use. It is
primarily prescribed to control abnormal heart rhythms (arrhythmias).
The total daily dose of Quinidine in this study is less than one tenth
of the dose normally used to treat arrhythmias. Preliminary data
suggests that a combination of Dextromethorphan and Quinidine may reduce
uncontrolled expressions of emotionality in patients with ALS.
This phase II-III study was preceded by a small phase I study.
Study Design
The study is a double-blind, controlled, parallel, three-group study
comparing AVP-923 to its individual components (i.e., Dextromethorphan
alone and Quinidine alone) over a 29-day period. The total number of
subjects to be enrolled is approximately 100. Twice as many subjects
will receive the combination of Dextromethorphan plus Quinidine as will
receive either component alone. Enrollment is expected to last until the
Spring of 2002.
During the study, a small capsule is taken orally, two
times a day (every 12 hours). AVP-923 is generally well-tolerated.
Possible side effects include fatigue, dizziness, euphoria, confusion, rash, or diarrhea.
It is hypothesized that AVP-923 will reduce the frequency
and/or severity of uncontrolled laughing and/or crying episodes. Over
the course of the 29-day trial, frequency and severity of pseudobulbar
affect, quality of relationships, quality of life, as well as standard
physical measures will be assessed. Participation in the trial will
require one visit to establish eligibility for the trial and then 3 more
visits during the 29-day trial period.
AVP-923 is an investigational drug for the treatment of
pseudobulbar affect in ALS. Unexpected adverse effects can occur. If you
are not enrolled in the AVP-923 clinical drug trial, do not take
dextromethorphan and quinidine without consulting with your physician or
other health care provider.
THE LASTING EFFECTS OF DXM
A PERSONAL EXPERIENCE
by temoku
I quit doing DXM 8 months ago. I was doing it about once to twice per
week and an average of about 800mg, going up to 1000mg a few times (I
weigh 150lbs). Some of you may be interested in how I've experienced the
past 8 months. To begin with DXM is awesome, or I think so anyway, but I
would much prefer to have full mental functionality for this lifetime
than a few fun
trips. Here is how DXM has affected every aspect of the experience of my life for the last 8 months:
First 3 months:
Constantly felt extremely detached from my surroundings. So much so
that I often times was unaware of what my body was doing i.e. I found
myself doing stupid things like waving my hands around (like you do when
trying to dry them) but only realized it after I'd been doing that for
some time (20 minutes or so I'm not sure of how long). Paralyzed with
anxiety and fear,I developed my own version of what was going on in my
surroundings based on this anxiety and then reacted to what was
happening in my mind as if it were actually happening outside of me
(which of course it wasn't as the people in my life can confirm). This
along with the fact that I could not tell that there was a difference
from me an another person made me start thinking I was schizophrenic.
The weirdest part is I can't see properly; you know when you are on DXM
and you are seeing something (like the door or a wall) and you know you
are seeing it but it doesn't seem like you are looking through your eyes
(kind like you are hovering just about your head or something)? Well my
vision was like that, everything was surreal and I mostly saw things
like what you see when you look at the american flag for 10 minutes then
close youre eyes. It took effort to look at an actual object.
5 months after quitting DXM:
Only just being able to tell that there is a difference between me and
another person, anxiety getting better, vision much better but very
spatially disoriented. In other words: sometimes I would look at
something and it looked like there was no space between me and what I
was looking at, almost like the world was 2D. Very very strange. Oh and
by the way, I was in school studying visual basic and Java programming
languages and finding my once well honed logical thinking skills were
suffering.
Where I am now:
I feel very close to normal now, almost no anxiety, able to carry out
a conversation with someone and feel the great relief and joy for the
fact that they are NOT me!! The most prominent thing now is the spatial
disorientation. I still have a hard time with anything 3D, like building
a fence or a room or something. Also the anxiety floods back in every
now and then. And I'm definitely not quite as sharp on some things as I
was previously but fortunately those things are few. I remain confident
that I will be able to become a good C++ programmer (and my grades
reflect that)!
You can reach this individual at [email protected].
ANOTHER PERSONAL EXPERIENCE
by Jacy
For around 2-3 months after taking DXM several times, I felt 'cloudy'.
My brain just did not feel as 'crisp' as it did before. I was unable to
understand or do any complex logical work (eg my job programming). I
dont know if I could feel it physically, but in a sense I could
definitely *feel* that something was different. I was worried that I had
gotten brain lesions from my usage, and stopped using for a few months.
Over those next few months the feeling passed and I believe my brain is
operating at almost full potential again. I dont think I have recovered
100%, but in the range 90-95%.
I dont know if anyone else has experienced this. I am definitely not
imagining it all tho.
On a side note (sort of), other prolonged effects from
acid (I think) includes: visual trails, seeing things in shadows, having
to spin around all the time because I think someone is behind me.
Sometimes I just get the physical feelings I am on acid (back of head
hurts, throat and body feels weird), even tho I havent taken any
in over 3 months now.
You can contact this individual at [email protected].
THE DXM BIRTH-DEFECT SCARE
 THE SCARE THAT RESULTED FROM "DEFECTED" RESEARCH
THE SCARE THAT RESULTED FROM "DEFECTED" RESEARCH
by gravol
The following information is from Wide Smiles (http://www.widesmiles.org),
and has been disputed by most every physician because of its flawed
research using chicken embryos, which are extremely unreliable. However,
if one is pregnant, one should not be using any kind of recreational
drug to begin with. The following is the report as it came to us:
WESTPORT (Reuters) -- Dextromethorphan, an ingredient in some cough
medicines, has been shown to cause birth defects and fetal death in
chicken embryos exposed to concentrations relative to those typically
taken by humans, according to a paper in the January issue of Pediatric
Research.
Dr. Thomas H. Rosenquist and colleagues at the University of
Nebraska gave chicken embryos various doses (5, 50 or 500
nanomoles/deciliter) of dextromethorphan over three consecutive days.
More than half of those given the highest dose died, while about
one-eighth of the survivors developed congenital defects including
"..neural tube defects such as spina bifida, facial defects similar to
cleft palate, as well as cranial defects," a University press release
explains.
"Dextromethorphan was also highly lethal at 50
nmol/embryo/d," the team writes in the Pediatric Research paper.
According to Rosenquist, these findings add weight to
recently reported findings from the Baltimore-Washington Infant Study in
which a history of cough medicine use emerged as a risk factor for
congenital malformations.
"We found that dextromethorphan causes defects so early
in the development of the embryo that in many cases the woman wouldn't
even know she is pregnant," Rosenquist said in the statement. "We feel
that a single dose is capable of causing a birth defect and that,
ultimately, it could be the cause for a woman to have a miscarriage."
Dextromethorphan suppresses cough by acting on receptors
in the adult central nervous system. But in embryos, the drug appears to
"knock out" the receptors, thus leading to the defects.
Further study is needed, but in the meantime, Rosenquist
suggests that pregnant women be advised not to use
dextromethorphan-containing cough medicine.
"Although we used chicken embryos in our study, modern
molecular biology shows that the same genes regulate early development
in virtually all species -- from insects to worms to humans," said
Rosenquist. "Based on this, it can be predicted that the effects
dextromethorphan had on the chicken embryos also would occur in human
babies."
It
should be noted that this study was published in 1998 and no other
studies have been published since then backing up this claim.
A DXM NIGHTMARE
 ONE BOYFRIEND'S PLEA FOR DEALERS TO STOP DISTRIBUTING DXM POWDER
ONE BOYFRIEND'S PLEA FOR DEALERS TO STOP DISTRIBUTING DXM POWDER
Exclusive by gravol
On June 22 on the Usenet newsgroup alt.drugs.psychedelics, a frantic
plea came in from a very distraught boyfriend. The following is what was
posted by that boyfriend, DAREzombie:
"I live in vermont, and some idiot provided my 15 year old ex
girlfriend with 600mg of dxm, and she found out the hard way she's 2d6
deficient. Long story short, she ended up in the hospital for the past 4
or 5 days, and can't even remember her name or where she is when she
wakes up in the morning. In her DXM induced ramblings she ratted out
EVERYONE in my town, all the dealers, everyone she's smoked pot with.
The cops have been trying to put wires on everyone they bust, and it's
all because some clueless idiot decided to make a few bucks selling a
chemical they had no fucking clue about to a young clueless girl that
wanted to get fucked up."
She had no sitter because she had no idea how powerful
the shit is. The kid that hooked her up with it said that if you take 2
of the 300mg pills (which is a stupid dose per pill.. whoever bought
this shit and set it all up for sale was apparently an absolute idiot)."
She was in the hospital for days for a reason, she was
totally blacked out for 2 days (in which she ratted everyone out) and
she lost vision in her right eye for 3 days, and she was having seizures
and uneven breathing. I talked to her today and she's still a little
confused and gets dizzy just from standing too long. I told her
everyone's pissed at her because she ratted everyone out (in a 1 1/2
page tellall confession with names up the ass), and at first she totally
denied doing it, and then all of a sudden realized she did and started
crying. And btw it was her mom that brought her to the hospital when she
started having seizures and kept saying she was blind. fucked up shit"
The female
in question weighs about 115 to 120 pounds and is only 15 years old. The
hospital had diagnosed her as literally blind in one eye but it slowly
came back after the 2nd or 3rd day. None of this has been substantiated,
but we are accepting this person's report at face value. It provides a
nightmarish perspective into the world of those who try DXM and find
themselves to be deficient in the enzyme that metabolizes DXM. We will
continue to update you on her progress in future issues.
A BRIEF SYNOPSIS OF DXM AS A DISSOCIATIVE
AND A CLOSER LOOK AT THE PROPERTIES AND CLASSIFICATIONS OF DXM
by gravol
Introduction
Notice the similar structural formulas for PCP, ketamine, and DXM. All
three drugs each have one benzene ring and in the case of PCP and DXM
both have one carbon ring. DXM's structure is also very similar to that
of levorphanol, with the *only* difference being an extra methyl group
instead of an HO (perhaps levorphanol in high doses also exerts a
dissociative effect?).
Properties
Dextromethorphan, which is
(+)-3-methoxy-17-methyl-9a,13a,14a-morphinan, is the methyl ether of the
dextrorotatory isomer of levorphanol, which latter is a narcotic
analgesic and from which DXM can be synthesized by methylation of the
phenolic hydroxyl group (U.S. Patent 2,676,177, issued in 1954).
The name dextromethorphan is broken down by prefixes and
suffixes. Dextro- means of the right, meaning the right isomer of
levorphanol, and -meth refers to of the methyl group, since DXM has an
extra methyl group that levorphanol doesn't. The last part of the name
actually refers to the drug methorphan, which is a methyl analogue of
racemorphan, as codeine is of morphine. DXM is the right isomer of
levorphanol as levomethorphan (LVM) is the left isomer, and may also
have dissociative properties, but unfortunately this chemical has long
since been banned
History
Dextromethorphan HBr was first prepared by Grussmer Schnider while
working for Hoffmann-LaRoche. Being an opiate it is considered a
controlled substance listed in the U.S. Code of Federal Regulations,
Title 21 Part 1308.12 (1987); however for over 40 years it has remained a
unique psychedelic and one of the single best legal ones
available. In fact, according to the American Journal of Medical Science
(227, 291; 1954) it is of equal antitussive effectiveness as codeine.
As
recently as 1971, the drug was still under close scrutiny by the Council
on Drugs of the American Medical Association, which stated that final
assessment of its antitussive efficacy and relative potency must await
results of objective clinical trials.
The brand names for DXM when it first appeared in the 1950s were Methorate (Roerig) and Romilar (Sauter).
DXM as a Narcotic Antitussive Analgesic?
To many people, DXM is many things. According to Henry Hitner, Ph.D.,
who is the Vice Chairman of the Dept. of Physiology and Pharmacology of
the Philadelphia College of Osteopathic Medicine, and Barbara Nagle,
Ph.D., who is the Director of Program Planning and the Medical and
Pharmacy Education Director of III Associates in Bryn Mawr, PA, and
according to the Glencoe Basic Pharmacology Textbook (4th ed., 1999),
DXM is a Narcotic Antitussive.
The book states (pp. 220-222, 223) that "Certain narcotic
analgesics (codeine and dextromethorphan) are antitussive (suppress
coughing). In general, the antitussive analgesics are much less potent
analgesics than morphine and possess a lower addiction liability.
Therefore, codeine and dextromethorphan are considered relatively safe
and are frequently found in over-the-counter remedies."
It should be interesting to note that the majority of
doctors and the companies that manufacture DXM do not promote the drug
as a narcotic; however, the above doctors and most pharmacology
textbooks show DXM as a "narcotic antitussive analgesic."
DXM as a Psychedelic?
There is even less medical information available regarding DXM as a
psychedelic. The term "psychedelic" first appeared in 1956, and is in
close conjunction with a hallucinogenic drug. In fact, the term
psychedelic is not used in medicine, but is instead referred to as
hallucinogenic/psychotomimetic.
There is much debate whether DXM is a true psychedelic,
as is LSD. However, most anyone who has taken DXM in large-enough
dosages agrees that the drug is not only a hallucinogenic but a
psychedelic as well.
The characteristics of a psychedelic drug is simply a
drug that causes A) sensory distortions, B) pseudohallucinations, C)
perceptual distortions, and possible D) dissociation. The only category
DXM does not fit under that is common of most hallucinogenic drugs is
that it is not a CNS stimulant. However, under the common defintion of a
psychedelic, it is not stated that for a drug to be a psychedelic it
must stimulate the central nervous system.
As for the other characteristics of psychedelics, DXM
does cause sensory distortions (merging or floating into the back of a
chair), pseudohallucinations (closed-eye visuals), perceptual
distortions (the slowing down of time) and dissociation (feelings of
separation of part of the body, or loss of a part of the body, or
failure to recognize a part as one's own body). In fact, most people who
use DXM on a regular basis do classify it as a psychedelic. Just
because DXM doesn't neatly fit into any certain category (LSD-like,
tryptamines, and phenethylamines) of psychedelics doesn't mean that it
is not a psychedelic. In fact, DXM doesn't neatly fit into any category
of any drug. Its actions are five times the complexity of marijuana.
DXM as a Dissociative
DXM is most commonly known as a dissociative. As stated before, it has
a similar structure to that of PCP, and has even been referred to as
"poor man's PCP."
And like the characteristic of most dissociatives, DXM is
being used in post-operative surgery as a general anesthetic.
DXM exerts its dissociative action by binding to the NMDA
receptor site and plugging it up, just like PCP and ketamine does. It
is known that ketamine inhibits NMDA receptors by two mechanisms by a
blockade of the open channel by occupying a site within the channel in
the receptor protein, and a reduction in the frequency of NMDA channel
opening by drug binding to a second attachment site on the outside of
the receptor protein. Those are the exact same effects that DXM
produces, and PCP probably also shares this duality of action.
The NMDA blockade has to do with most of DXM's intoxicating and dissociative effects.
DXM and its Relationship with PCP
Phencyclidine (PCP) was investigated for use as a general anesthetic
in humans. It was developed in 1956 as a potent
analgesic-amnestic-anesthetic agent. It was briefly used as an
anesthetic in humans before being abandoned because of a high incidence
of bizarre and serious psychiatric reactions. However, because of a high
incidence of emergence delirium, it was dropped from further
consideration for this purpose. It is still used in veterinary practice
to immobilize primates. Like DXM, because of its psychotomimetic
effects, the drug has gained wide popularity as a drug of abuse.
Also like DXM, the pharmacology of PCP is complex.
Phencyclidine and dextromethorphan produce multiple pharmacological
actions, including CNS depression, peripheral autonomic effects,
analgesia, and anticonvulsant activity. The only difference between the
two is that PCP may also produce CNS stimulation as well as depression.
Phencyclidine interacts with several neurotransmitters, and
these interactions are known to account for many of the actions of PCP.
Much like DXM, the effects of PCP vary significantly with
increasing dosage. At low doses, there are CNS stimulation, euphoria,
and sympathetic stimulation similar to the effects produced by
amphetamines. With increasing dosage, thought processes become
disoriented and speech is slurred. This is followed by paresthesia,
slowed reflexes, and ataxia. Disorders of body image are common, with
both elongation and shrinkage of extremities. This state may last 4 to 6
hours, after which a depressive state occurs, along with a paranoid
behavior pattern. It may take several days before the affected
individual returns to normal.
DXM may also cause a false positive for PCP, which is
quite common, and because of this, a positive assay requires secondary
confirmation. One case involved a blood test showing a possitive assay
for PCP after ingestion of dextromethorphan powder.
As you can see, the effects of PCP and DXM are different
from another. However, in a general sense, DXM is similar to PCP. More
similar than DXM is to most drugs, including other narcotic analgesics.
The dissociative effects are actually a lot closer to those of ketamine.
DXM and its Relationship with Ketamine
Ketamine was first synthesized in 1964 in Belgium (see Patent
634,208). According to the United States Dispensatory (27th ed., 1973),
"Ketamine hydrochloride is a rapid-acting general anesthetic that
produces a dissociative state of the central nervous system in which
amnesia and profound analgesia are induced although the patient does not
appear to be asleep." This is very similar to the effects of DXM in
high dosages.
"The compound is neither a barbiturate nor a narcotic, and
its action is quite different from that of conventional anesthetics."
The only main difference between DXM and ketamine is that ketamine is
short-acting and DXM is long-acting.
The psychological effects of ketamine include
pleasant dream-like states, vivid imagery, hallucinations, along with
possible confusion, excitement, and irrational behavior. This state is
very similar to the dissociative action of DXM.
Ketamine is still occasionally used in humans to
provide anesthesia in patients who cannot tolerate the cardiovascular
depressant effects of other anesthetics, and DXM is likewise being used
in high dosages for post-operative surgery.
DXM as an Antidepressant?
William White states that "The music euphoria and motion euphoria are
probably partly due to PCP2 activity, and partly due to other activity.
As NMDA blockade and sigma activity can both lead to dopaminergic
activity, reuptake inhibition would potentiate these effects.
"Interestingly, DXM seems to be much more potent at this
site than other sigma/NMDA ligands (such as PCP or ketamine) in
comparison to activity at other sites. Also interestingly, at least one
tricyclic antidepressant has been found to be active at related
receptors (sigma, PCP); it is possible that the PCP2 site may be a
target of some antidepressants."
This makes the case for some that DXM also has
antidepressant action, but not by the reuptake of serotonin, in the
traditional sense.
Metabolism of DXM and Grapefruit Juice
DXM enters the bloodstream through the GI tract within 30 minutes. It
is ultimately metabolized to 3-hydroxymorphinan (3HM). DXM is converted
to dextrorphan (DXO) by a liver enzyme called cytochrome P450-2D6
(debrisoquine 4-hydroxylase). This is the same enzyme that metabolizes
caffeine and other drugs. One thing William White failed to note, is
that by ingesting grapefruit juice (GFJ), which contains naringin, it
greatly alters and prolongs the metabolization of DXM, and may lead to a
more euphoric effect.
Conclusion
DXM is very similar in both properties and effects to other
dissociatives, like PCP and ketamine. One sidenote is that there are
many more dissociatives, which are inhaled. Nitrous oxide (N2O), for
instance, is a powerful anesthetic and dissociative. The combination of
N2O and DXM can be quite a euphoric experience. However, DXM is most
similar to PCP and ketamine in both effects and its action on NDMA
receptor sites.
DXM stands alone in that it is both legal (though regulated
by the federal government) and hallucinogenic. The most common trait of
DXM is its dissociative action, and thus should be classified as a
dissociative at higher dosages, and as an antitussive in lower dosages.
DXM AND DREAM RESEARCH
 EXCERPTS FROM THE DREAMING FAQ REGARDING DXM
EXCERPTS FROM THE DREAMING FAQ REGARDING DXM
by Rob Bowling, Pharm.D.,Ph.D.
The first anecdotal reports of Dextromethorphan have been around since
the early 1960s, although it's use was then by those in the medical
community.If you FOIA the original NDA materials for Dextromethorphan to
the predecessor to the FDA, you will notice that these indicated that
Dextromethorphan had possible addiction potential. It was *never*
kept secret in the industry, or in the government.Just as Tiletamine
(which is *only* controlled federally *as a combination product*), and
Ketamine (before it became a Controlled Substance) many ofthese
substances weren't considered a real concern because of drug delivery
systems, or because of other reasons, even though the medical community
knewof their possible abuse and addiction qualities. With
Dextromethorphan, it was a matter of formulation: syrup formulations
back then. And, most believed that because the studies which they
relied on indicated that witheven moderate doses, the effects of
Dextromethorphan on the Chemorecptor Trigger Zone (the area of the brain
which controls nausea), overdose issues would not be an issue for the
population at large. The "information" about Dextromethophan being a
"recreational drug" thatfirst started appearing on BBS's in the
mid/early 1980s came fromlittle-known "home grown" books published in
the early 1970s for the most part. This information came from
those who had used it in the 1960s. There have always been rumors that
even some of those in the development of Dextromethorphan tried it
recreationally (although this is more than likely an urban legend).But,
you are still correct that Guifenesin in cough syrup predates the
recreational use of Dextromethorphan. However, many in the medical
community still argue that it is of questionable efficacy used
incombination with Dextromethorphan, or any cough suppressant for that
matter.
----
1.5. Do substances like drugs, herbs and foods affect our dreams?
Yes
. During REM protein-synthesis is highly active, so your body needs
highlevels of amino acids. The neurotransmitter in use during REM is
Acetylcholine. It is made from the B-vitamin Choline and the vitamin
B-5.But there are more vitamins that can make us dream more. The body
can synthesis the B-vitamin Choline. But in order to do that it needs
vitamin B-12, Folic acid (B-9), the amino acids Methionine and Serine.
Vitamins B-12plays a role in the activation of amino acids during
protein formation. Ithas also the ability to increase the production of
Acetylcholine andnormalize neurotransmissions in the brain.Vitamin B-6
is another important vitamin. It is a co-enzyme, which participates in
over 60 enzymatic reactions involved in the metabolism of amino acids.
It is involved in the production of several body proteins and
neurotransmitters. It is particularly indispensable to the action of
aminoacid neurotransmitters, like Serotonin, Dopamine, Melatonin,
andNorepinephrine, which effect brain function. It is also involved in
themetabolism of Selenium, Calcium, and Magnesium. Melatonin is a
neurotransmitter/hormone that is only active during sleep. It is being
metabolized when you fall asleep from Serotonin, a neurotransmitter that
is being metabolized from the amino acid Tryptophan. Melatonin
increasesnon-REM sleep and makes it easier for you to fall asleep. But
it has also an interesting rebound effect that gives more frequent and
vivid dreams. The vividness might even give you a lucid dream.The amino
acid Tryptophan can be metabolized into Serotonin and Niacin
(B-3).Vitamin B-6 promotes this conversion. Taking Niacin or Nicotine
patches will increase the Serotonin production. The more Niacin you
take, the more Serotonin is produced and more Melatonin is metabolized.
Calcium and Magnesium promotes Serotonin production as well. Zinc is in
every cell of the body and is a part of over 200 enzymes, so Zinc
supplements may increase REM-sleep, too.DMAE (Dimethylaminoethanol) is a
very important B-vitamin. It flows easily through the brain's blood
barrier, where it is converted into Choline. During REM, Choline is
added the coenzyme A (Vitamin B-5), and we have Acetylcholine, the
neurotransmitter in use during REM. 5-HTP (5-Hydroxy-TryptoPhan) is a
Serotonin precursor that also flows quite easythrough the brain's blood
barrier. It is a good alternative to Melatonin.Vitamin C helps
metabolizing several amino acids and hormones. It is also important to
have adequate levels of amino acids. A few important ones are
Phenylalanine, Tyrosine, Methionine, Cysteine, Serine and Tryptophan.
Using Tobacco, Alcohol or Coffee prohibits the absorption of necessary
vitamins and amino acids. Depressants suppress REM sleep, one is
Alcohol, but taken in right doses can create a rebound effect so that
you wake up remembering many vivid dreams. And anti-depressants may
increase dream recall. Caffeine will make you sleep lighter, will
increase your dream recall and maybe even give you a lucid dream. Herbs
like Valerian, Mugwort, Mullein,Kava Kava, St. Johns Wort, Calea
Zacatechichi, Salvia Divinorum, Scutellaria Indica, Licorice Root,
Vervain, Jasmine, Honeysuckle, Datura, Bee Pollen,Catnip, Hops,
Scullcap, Lavender, Damiana, Withania Somnifera, Passionflower,
Chamomile, Cardamom, Gotu Kola, Ginkgo Biloba, Ibogaine, Verbena,
Rose,Cinnamon, Marigold, Nutmeg, Peppermint, Holly, Yarrow and Anise may
help youdream more, recall more or even have a Lucid Dream. Make sure
you know moreabout these herbs before you use them: some are to be used
in pillows, someare to be smoked, some are to be used in tea, etc. And
finally we have psychedelic drugs like DXM that may induce Lucid Dreams.
Some of the drugs and herbs can be addictive, and be poisonous if taken
in too large doses. Crystals and Magnets may also affect your dreams.
TESTIMONIALS OF PEOPLE WHO USE DXM FOR LUCID DREAMING AND OUT-OF-BODY EXPERIENCES
compiled by gravol
Jacob Jarnigon:
You know when you're about to have the obe when your body tingles or
loud vibrations pulsate throughout. Sometimes I get excited and wake up,
that sucks! Really, I've been having somescary problems though. When I
go obe there has been these things grabbing me and slinging me
around; sometimes they drag me into theground, way down, it's another
world it feels like. I've learned they won't hurt me but are just having
fun with me. The funny thing is thishas been going on for a while, but
just recently there has been some psychedelics (mainly DXM) that have
allowed for me to view their wavelength visually while I'm awake and now
I can see them (or they finally are showing themselves) while I'm ob;
that being the only way I can touch them physically. Their appearance is
simple: Imagine a 2ft long string with many mop-like strings hanging
from it ; that is aboutthe jist of their looks. I can't explain exactly
how they are because they are on a different wavelength. Nothing
we know can apply to these"whatevers" (as I call them). Nobody knows
about me and these whatevers. Just last night I was making love to
my girlfriend, totally sober, when they came up out of the ground to
watch, the little weirdos! I threw a pillow at one of them to try and
scare themoff and my girlfriend turned around and looked back at me
saying"what's wrong baby?" I replied, "nothing's wrong, you just feel
so,so,good." Anyways, they're harmless and my fear of them has gone. I
just want to say this: there are an indefinite amount of undiscovered
wavelengths, which could possibly (and probably do) comprise worlds as
real , if not more real, than our human world. They are undiscovered,
but real. Nobody is crazy, just perceptive. Most psychedelics can
stimulating actual lucid dreams. And DXM usually makes people
drowsy enough to go to sleep. A DXM, or ketamine experience can very
closely resemble theact of lucid dreaming. When you go into a dark room
or close your eyes on these two substances you leave your body and enter
3 dimensional hallucinatory worlds.
CTSaen ( [email protected] ):
Well to start off I am in NO means advocating this method..but it
works for me so here goes. I have been a frequent lucid dreamer
since I was very young. But I could never control the onset of these
dreams. Also I had never beenable to achieve an OBE...I have come
close but there was always something blocking the exit or I would fall
asleep trying. Recently, I have discovered
DXM..Dextromethorphan...I took approx...350 mg. And I was feeling
light headed about two hours after taking it...I laid down and tried to
fall alseep...I wokeup dreaming...instantly became lucid...VERY
VIVID...I woke up...to realize Iwas peaking on the DXM...rolled to the
my other side...and BAM...blasted out of my body..and turned to see my
face staring in horror...VERY SCARY...suddenly my room went black and a
tunnel appeared before me...I heard whooshing sounds and was sucked into
this tunnel..where I returned to the lucid dreamscape I had just been
in...the dreams lasted much longer then normal...I explored the astral
plane..met dead relatives..and met spirit guides...then Id feel a pulse
in my consciousness..and id be yanked back at tremendous speed back to
my body...this process continued several times during the night..I didnt
seem tohave control of return or seperation...it was very
disconcerting..but while Iwas in the astral...I did have control over
that environment etc...i would be interested to know if anyone else has
had similar experiences...Thanks
Clarity Now! ( [email protected] ):
The DXM "oobe" is not the same as a what most folks in this newsgroup
are striving for -- being able to explore other dimensions without
theuse of drugs. (I could be wrong!) For the main part, DXM causes
psychedelic hallucinations -- it's chemically induced. You have
no real control, but I"m sure there aretimes you think you do.
DXM is great if you aren't able to get OOB naturally and are
frustrated. I've tried it at the upper plateau levels and the
experiences were definitely memorable. My favorite part is flying
through space at light speed :) I've also had what seem to be
psychedelic visuals (I've never tried LSD, so I don't know) -- but
pillows of jel-like globs of color coming at me (now I know where the
inspiration for lava lamps comes from .) I guess you could take
this to the alt.drugs.psychedelic ng to seewhat others have to say about
such an experience.
Anonymous:
I haven't read many accounts of this outside the DXM FAQ trip report
section, but a handful of times I combined DXM with other psychedelics.
DXM+psilocybin, DXM+LSD, were both spectacular memorable
experiences. Although DXM is not "visual" in the same way as
psilocybin or LSD when I combined them I saw very detailed geometric
patterns, and have had many interesting experiences on DXM with and
without other drugs with eidetic imagery and hypnagogic
landscape-flying...
THE DXM ENIGMA - THE PYRAMIDS AND 11:11

AND HOW IT COULD AFFECT YOU
by Anonymous
[Editor's Note:
It's not that the writer of this wishes to remain anonymous, but I
have lost the information pertaining to his identity. However, I feel it
is relevant enough to post anyway. For those of you who are confused
about the 11:11 phenomenon, you can visit http://www.nvisible.com/1111.htm
and learn more about it there. In brief, 11:11 affects many people,
the majority of which have not even heard of DXM. It affects doctors,
scientists, religious people; it does not discriminate. We believe it is
a wakeup call of things to come in our lifetime. So please do not take
the following information lightly, especially if you have witnessed this
strange phemonenon.]
On Aug. 11, on grid point 11 at 11:11 a.m., the Solar Eclipse went
into complete corona, where the hyperdimensional energies of the Sun and
Moon were as precisely aligned as they could ever possibly get. And, as
we had said in the previous edition of this book, finished March 8,
1999:
With all the attending stresses of the Grand Cross
configuration, this Eclipse will become as a laser beam of focused,
fourth-dimensional consciousness/energy, or metaphorically significant
as the lance that pierced the body of Christ on the Cross. As this
hyperdimensional "laser beam" reaches its strongest point of corona, it
also ignites one of the most highly significant Grid vortices on Earth -
the location of Stonehenge and a host of other megalithic stoneworks.
This single burst of energy will blast the Global Grid so strongly that
the entire Grid itself will sound like a gigantic gong, rising to an
incredible height of frequency for a few moments�We can also expect that
this blast of energy would continue to cause the Global Grid to expand,
thereby causing land shifts as Wilcock's readings are predicting.
And indeed, on Aug. 17, 1999, the exact day when the
Grand Square planetary conjunction itself went into its tightest
alignment, there was a tremendous 6.9 earthquake in Turkey -- directly
over the area where the eclipse path had traversed just six days
earlier. This was all the convincing that was necessary to see that
these effects really can be measured and predicted. Taiwan then followed
soon afterwards with equal severity. We remember seeing the ring of
energy created in the Pacific Ocean basin, and how much it resembled
cell mitosis, as though the Earth itself was showing us a physical
metaphor of regeneration. We also remember Joseph Jochmans' information
from Athelsan Spilhaus and others that suggests that such a geometric
expansion has already occurred in the past. The Hopi prophecies about
the Earth's grid expanding like the white spots on a growing doe are
also very interesting bits of corroboration.
So, this continuing increase of Light or aether density
into the global energy grid, by such a precise hyperdimensional
arrangement of forces in the galaxy, cannot go without its effects. The
Ra Material tells us that the Earth will have to "electromagnetically
realign its vortices of reception," and that they have "every reason to
believe" that the sum total of this realignment will be approximately 20
degrees due east of North. Furthermore, there is even more intriguing
research to show that the "gateway" of 11:11, which opened on Aug. 11,
1999, had great significance. In Graham Hancock and Robert Bauval's
book, Message of the Sphinx, [or Keeper of Genesis in Europe,] the 11:11
ratio is specifically mentioned as being of quintessential importance
to the functioning of the entire pyramid itself! This 11:11 ratio
is also shown to have a harmonic connection to the angle measurement of
111.111 degrees, elsewhere in the Gizeh complex.
In Hancock and Bauval's work, there are frequent
citations from the landmark Pyramid Texts of Unas, and their reference
to the First Time, or "Zep Tepi." Hancock and Bauval tell us that this
First Time of Egypt was 12,500 years ago, the exact date of the close of
the most recent Solar Breath / precessional cycle. At this moment, the
point where the Sun would rise, called the vernal point, was directly in
front of the Sphinx within the constellation Leo, the Lion. Hence
the very first thing we see is how the terrestrial Sphinx was built to
face its celestial counterpart. This obviously is another piece of
evidence linking the Sphinx to a time of 12,500 years in the past.
This Sphinx alignment dovetails nicely with Bauval's
discovery that the three pyramids of Gizeh are a precise terrestrial map
of the constellation Orion, designed to be in exact alignment with the
celestial Orion 12,500 years ago. Then, we are told that the second
major time-encoded date for the Pyramid complex is the point at which
the internal "airshafts" in the Pyramid align with their celestial
counterparts in the heavens. The time where everything fits
together is in 2500 BC, almost exactly 8000 years after the First Time
of 10,500 BC. The vernal point, where the Sun rose, has then moved
exactly 111.111 degrees away from where it started in 10,500 BC! There
again, we have an apparently built-in, deliberate numerical
synchronicity showing itself!
Hancock and Bauval speculate that the pyramids might
somehow be able to facilitate time travel within the focus of
consciousness, so that those of the Egyptian Pyramid Age might be able
to scan backwards to this "First Time" of 12,500 years ago. If this is
true, then they suggest that these precision alignments in the Pyramid
have their purpose for calibrating that specific time. The reader will
remember that we discussed similar methods of time calibration in the
chapter on the Constant of Nineveh. Thus, on page 235 of "Message of the
Sphinx," they write that since the precession causes a one-degree shift
every 72 years,
�If the Horus - King could have been provided with the
'special number' 111.111, and had used it in the way described above, it
would have led him back to (72x111.111 years =) 7,999.99 years before
the specified 'ground zero,' i.e. to almost exactly 8000 years before
2500 BC - in short, to 10,500 BC.
We know that this seems like wishful numerology of the
worst sort - i.e. 'factoring in' an arbitrary value to a set of
calculations so as to procure spurious 'corroboration' for a specific
desired date (in this case the date of 10,500 BC, twelve and a half
thousand years before the present...) The problem, however, is that the
number 111.111 may well not be an arbitrary value. At any rate, it
has long been recognized that the main numerical factor in the design
of the Great Pyramid, and indeed of the Giza necropolis as a whole, is
the prime number 11 - a prime number being one that is only divisible by
itself to produce the whole number 1. Thus 11 divided by 11, i.e.
the ratio 11:11, produces the whole number 1 (while 11 divided by
anything else, i.e. any other ratio, would, of necessity, generate a
fraction.)
What is intriguing is the way that the architecture of the
Great Pyramid responds to the number 11 when it is divided, or
multiplied, by other whole numbers. The reader will recall, for example,
that its side length of just over 755 feet is equivalent to 440
Egyptian royal cubits - i.e. 11 times 40 cubits. In addition, its
height to base ratio is 7:11. The slope ratio of its sides is
14:11 (tan 51 degrees 50'). And the slope ratio of the southern
shaft of the King's Chamber - the shaft that was targeted on Orion's
belt in 2500 BC - is 11:11 (tan 45 degrees).
Arguably, therefore, the ratio 11:11, which integrates
with our "special number" 111.111, could be considered as a sort of
mathematical key, or 'stargate' to Orion's belt. Moreover, as we
shall see, a movement of 111.111 degrees backwards along the ecliptic
from 'ground - zero' at the Hyades - Taurus, the head of the celestial
bull, would place the vernal point 'underneath' the cosmic lion."
So now we can see that Hancock and Bauval directly
mention the 11:11 ratio as the "stargate" of the Great Pyramid! [Note:
Just as this book is in its final edit and going to print, a huge bolt
of lightning exploded overhead in a giant flash, right as we read the
word "Stargate" again.] Synchronistically enough, the colon between the
two numbers, which indicates a ratio, reads exactly the same as the
colon in clock time, AND exactly the same as the colon in Bible
quotations! This lends even greater credence to the validity of the
11:11 conjunction being so important - it appears that the entire
Pyramid was built to encapsulate this number! Then, when we see the
focus on the internal timelines, the metaphor of the returning capstone
and the Masonic connections of this symbol to "A great order of ages"
being "born anew," we must start to seriously consider that the period
between the Aug. 11, 1999 conjunction and May 28, 2000 conjunction will
end up being seen as a symbolic event of incredible significance to us
as a planetary species. The ancients clearly were able to focus in on
this time as being of significance, and in order for us to see it we may
need to study more of the "subtle" effects in society, such as the
changes in paradigms that are now occurring with events such as a major
motion picture about the Martian Anomalies.
We rounded out the book with a discussion of the Nineveh
Constant, which helped to show us how these cycles of time might be used
by extradimensional travelers to navigate through the timestream, or
the fabric of space and time. We also were given another glaring clue as
to the elegant beauty and simplicity of the harmonic numbers underlying
all of the Creation. Simply multiplying 70 by 60 seven times in a row
can render the entire Cycle, measured in seconds. The pulsar B1257+10
shows an almost exact similarity to our own in its configuration, and as
this is the first major extra-planetary system that we have found, we
can assume that they all function to some degree of harmonic
consistency. And with Wilcock's original research, this same harmonic
system has been expanded out to the Galactic level, and we can see that
all truly does work in perfect mathematical harmony.
With the work of Cowan and Masson, we see that time
itself takes on a dynamic, shifting, energetic structure that can be
accurately predicted in advance, and whose behaviors have certain
definite effects upon civilization. So now, we have an even greater
grasp of how our own Great Solar Cycle affects us as a planetary
society. (4:44 p.m., 3/8/98.) As we learn and understand the physics
behind the Shift of the Ages, we are made pure with our own realization
that all things are in balance. Whether we look at sound, color,
geometry, atoms, cells, biology, the human body, pyramids, the Global
Grid, planetary orbits, the Sunspot Cycle or even greater cycles such as
that of the Constant of Nineveh, and now the rise and decline of
massive, seemingly random social trends as well, we can see that all
things, indeed everything, obeys these magnificent, cyclical harmonic
principles.
We now know that a massive effort was made by the survivors
of the Atlantean cataclysm to preserve the basis of this knowledge for
our own generation. Mythologies the world over have encoded the
precessional numbers in their roots, and various other societies have
retained immense pieces of the puzzle, such as the Maya, the Aztecs and
the Sumerians. These teachings found their way into the Western secret
societies over time, and now they continue to thrive in the United
States Government and its backbone of Masonic belief, as well as the
United Nations as a whole in their remarkable Meditation Room.
We have also seen how the extraterrestrial forces
surrounding us at this time have made numerous efforts to communicate
these simple truths to us, through Nostradamus, Cayce, Jane Roberts,
Walter Russell, David Wilcock and others. We have indeed arrived at this
Omega Point of planetary Ascension now, and we are surrounded by a
throng of spectators. These brothers and sisters on the outside made
sure that we would have the necessary technology in place at the end of
this cycle so that we may process our collective karma from the Age of
Atlantis. It is time for us to Ascend, to regain our true heritage and
to reclaim the Earth, or the New Jerusalem, in its cleansed and
perfected fourth-density form. We have all the proof that we need to
convince ourselves that this epic, fantastic event is very soon to
occur.
THE HOW'S AND WHY'S OF CEV'S
 AN IN-DEPTH LOOK AT WHAT THE UNDERLYING CAUSES OF CLOSED-EYE VISUALS MAY BE
AN IN-DEPTH LOOK AT WHAT THE UNDERLYING CAUSES OF CLOSED-EYE VISUALS MAY BE
Exclusive by gravol
One of the greatest things I've ever experienced while tripping on DXM
was the presence of CEVs (closed eye visuals). In the last issue, I
went into some depth about what I experienced and saw in these visuals,
along with what is common to see. But now I feel I have begun to unlock
the door as to why some people experience them and others don't, and why
those that do experience them enough times only find them to dissipate
over time and occasionally come back, like some kind of magical spell
that whimsically eludes the follower.
The answer lies in the action of antihistamines, and how
they affect the brain. First of all, to help explain why antihistamines
are so important, are the following points:
1) Most CEVs are witnessed while under the influence of Coricidin
Cough & Cold, which contains the most powerful OTC antihistamine
available, chlorpheniramine maleate. The chlorpheniramine somehow causes
DXM to produce mind-boggling visuals of people, geometric shapes, and
other complex mathematical sequences when you close your eyes.
2) Another common antihistamine, diphenhydramine (Dramamine, Benadryl)
also occasionally produce DXM-like CEVs even when one is not under the
influence of DXM. Since most people do not mix DXM and this
antihistamine, it's rarely discovered. One safer alternative to viewing
CEVs without doing Coricidin is simply doing a dose of DXM after waking
up from a Benadryl nap - the likelihood of seeing CEVs is much higher.
3) In my
case, and in others that I have interviewed, CEVs are rarely seen in
just DXM itself, but for some people they are. Since antihistamines are
very common OTC drugs, a lot of people don't realize they may have
ingested an antihistamine within the past 12-24 hours of taking DXM.
4) The antihistamines themselves may not be what's causing the DXM -
you have to take an in-depth view as to how they affect your brain.
Perhaps low-histamine levels can greatly increase the occurrence of
CEVs. They are also not the only thing that precipitates the advent of
CEVs, but they surely produce the best results (see below).
So how do antihistamines work? Antihistamines generally, and
Diphenydramine Hcl specifically, act by antagonizing histamine at the
site of the H1 histamine receptor. Antihistamines dry up the secretion
of the nose, throat, and eyes. They relieve itch and will help you go to
sleep. Dimenhydrinate depresses the middle-ear function, but the way in
which it actually prevents nausea, vomiting, or dizziness is not known.
However, these drugs are not just antihistamines. They have a
significant amount of anticholinergic activity. What does this mean?
There's a chemical in the nervous system called acetylcholine, which is
one of a set of substances called neurotransmitters. These chemicals
transmit signals from one neuron to another. Acetylcholine is present in
many different parts of the brain. Notably, it's present in areas
thought to be associated with memory, and is the primary transmitter of
the motor pathways leading off from the spinal cord. It plays a role in
just about every system, however.
Acetylcholine is also the neurotransmitter in use during REM (dream)
sleep. Somehow these CEVs are linked to the same part of your brain that
regulates dreaming. And since dreams are still a total mystery to
science, chances are CEVs will be as well. But the answer could lie in
finding out more about the action of Acetylcholine and how DXM affects
its release.
Dramamine et al work to prevent acetylcholine from transmitting its
signals. The importance of acetycholine to memory may explain the
amnesia people usually have for the events during a high-dose Dramamine
trip. The heaviness that people often report is most likely a result of
the blocking of signals to muscles: the brain has to send a much
stronger signal to overcome the opposition produced by diphenhydramine,
and this is interpreted as a sensation of greater effort by the brain.
Now
with that in mind, perhaps acetycholine or lack thereof may something
to do with experiencing these CEVs. Surely, whatever is causing CEV
activity is affecting a very complex part of the brain, because the
visuals themselves are very complex. My guess is that the antihistamines
or some action they produce affects the NMDA receptor site or similar
sites, and cause these visuals (it may not have anything to do with NMDA
at all). Why would I say that? Because people have experienced similar
visuals on just antihistamines by themselves and on high doses of strong
narcotics (morphine, hydromorphone, etc), and there must be some common
link in how these drugs affect the mind that also works in a similar
way that DXM does when the conditions are right to experience CEVs.
If you want to maximize the occurrence of CEVs during
your trips, try the following - every one of these methods have been
proven to work in individual cases, however your mileage may vary.
1) Sodium chloride
- By taking a pinch or two of table salt before your trip, it
increases the chances of CEVs - while full-blown CEVs may not be
detected, the lines by which you can view them tend to stand out more.
This method has been tried by others with varying levels of success.
2) Brain vibration
- One very good method of greatly increasing your chance of CEVs
(this is the best method I have found as far as frequency and intensity
of CEVs) is sitting on a riding lawn mower (no push mowers - you have to
actually be ON one, riding on it) for at least 1 to 2 hours. This works
great if you happen to have a large lawn to mow, otherwise you have to
just bide your time on one - by being on something that is vibrating the
brain gets wrattled around a bit and the receptor sites are affected as
well - this would make a lot of sense. Unfortunately, riding in a car
does not do this because it doesn't vibrate.
3) Grapefruit juice (GFJ)
- One breakthrough that came to you exclusively by this Zine was the
advent of GFJ. It's now been proven that GFJ acts on the enzyme that
metabolizes DXM and slows down the metabolization. First-time users of
GFJ+DXM increase a high incidence of CEVs and a feeling as if it's your
first trip again. It's not sure how this may affect CEVs, except that
DXM stays in your system longer than normal. On the opposite note, the
new drug AVP-923 quickly speeds up the metabolization of DXM. Beware
that GFJ also potentiates many other drugs, like Xanax and Feldene, and
has led to many ODs because people were not aware of this fact.
I hope at least one of these methods will help you. The Zine does not
condone the use of DXM with antihistamines. We are very adament on this
stance, not to cover our ass, but to cover yours. Dramamine by itself is
fatal, let alone when mixed with other chemicals. And Coricidin is
probably responsible for the highest level of OTC overdose deaths
nationwide, though Tylenol probably causes more underlying liver damage.
Bottom line - stay away from Coricidin. The reason antihistamines were
brought up is to educate the reader on how and why CEVs are present for
some people and not for others, it's not a guide to maximize your own
CEVs (though the last three points may be used without any serious
incident).
What follows is a letter that was written by a DXM user who may be
conducting research in the future at the Beckman Institute regarding DXM
and CEVs:
I
did a 3rd-plateau dxm trip Friday night. I usually focus on the
closed-eye eidetic imagery (it is much more interesting than the
open-eye visuals). And so I found a very interesting phenomenon,
one that I'd seen before but not quite as lucidly as in this last trip.
Dxm
trips usually take off from whatever's been in your mind lately. It's
very set/setting dependent. So, there was a scene in my mind where
I was looking at a sort of "de-briefing room", like a war-room type
thing, with projector and secret codes on the screen, etc... I
guess this came from the fact that I've been playing Return to
Wolfenstein3d alot lately (and there are scenes like that here).
Only these scenes are a lot more lucid and detailed than
anything in the video games. Scrolling data pops up on the
projector screen, as people (or what I think are people) are moving
around in the background, all of this performed in real-time.
So on the screen, there seems to be a schematic printout
of a secret weapon, or some type of airplane. 3d drawing, rotating
on various axes, fully detailed.
For a moment, I wonder if my ability to influence the
eidetic imagery will affect such a lucid representation. So, just
out of the blue, I think of the most absurd thing I can, to test the
visualization, to see how robust this visualization system is... I think
of the word 'penis'
And within about half a second, I see the airplane *in
the projection* replaced by some sort or phallic shape. However, the
rotation is still going on, and the data output is still scrolling
alongside of it.
So I think 'typewriter' and the same thing happens.
Suddenly, a typewriter is inserted where the penis-thing was, and
yet the overall shape of the scene remains in tact. The people are
still acting as if they are looking at the information on the screen,
but that information is different. And, to top it all off, the
people themselves take on the shape of a typewriter (if that makes any
sense at all).
What fascinates me about his is the separation between
intentionality and content, between semantics and syntax. In
thinking of any particular word, it takes relatively little time (within
1 second) for the scene to change, and yet it isn't a complete scene
change, like a segue between two entirely differnet scenarios.
Instead, the new thought is inserted semantically into the
existing framework. If I am thinking of a certain person, that
person will suddenly appear, but not just pop up. Instead, he or
she will be incorporated into the current semantic context of the scene
(so instead of instantly appearing, perhaps he or she will walk into the
room, or something like that).
Another scence involved an item on a shelf underneath
what appeared to be a very large hat (again, I don't choose the nature
of the scene, only the semantic properties within it). Again, I
tested this phenomenon of choosing a particular semantic quality for the
scene. I remember thinking various different things, and they
would all show up underneath this hat. Then I remember thinking
'typewriter' (I don't know why 'typewriter' kept coming up), and I saw a
typewriter show up underneath this hat thing, slowly protruding, then
filling out the shape.
Then what was interesting was that the typewriter was too
big for the shelf, so the shelf collapsed. The mechanics of this
whole interaction were incredibly fluid, so much more than I could ever
have anticipated. Basically, the scene took what it saw as a literal
representation of what it would have seen in the external world.
It must have thought that if a typewriter were really there, it
would have been too heavy for it to stay up on the shelf, and so the
shelf collapsed.
What interests me in all these cases is the level of
semantic insertion into the scene. Like I said before, it wasn't a
simple replacement of one item or another, like a meaningless canvas or
visual playground. Instead, the scene attempted to maintain some type
of cohesion... When I though of a new concept, it was *inserted* into
the pre-existing semantic context. Perhaps the overall semantic
flavor of the scene was absurd, but at a lower level, the scene could
have made sense.
That is to say, the scene maintained syntactic integrity,
at least based on a certain visual 'synatax' (I remember speaking
with Brian about possibly doing my senior project on a sort of visual
syntax; he though it was too difficult a concept to do at the undergrad
level).
This is the type of research that I like to perform under
these various states. Determine what the level of representational
scope might be for whatever phenomenon I might be observering (in this
case, semantic insertion and syntactic cohesion), and see whether these
phenomena are applicable outside of the particular psychedelic state.
One could always simply complain that these are select cases
or phenomena that are only evident in these particular alterations of
consciousness. That is where you have to do more tests, to
determine what conditions are indeed constant, and what conditions are
anomalies presented by the alterations in consciousness.
There are other phenomena that I am quite interested in
under these states. For instance, what is the visual granularity
of eidetic imagery. In other words, how fine is the resolution of
this type of imagery. This goes into the aspects of underlying
representation. Not only that, what is the granularity of motion
of these images? In one scene, I was thinking about blood flow out
from a vein into a tube (I had just recently given blood), and I
had a full representation of the phenomenon in mind. I tried
slowing down the blood flow to its very slowest, and at that point I was
able to see individual 'points' of blood moving down the tube.
What I noticed what that these points sort of 'jumped' around at
such fine resolutions (that is, they didn't move continuously, but moved
more like if the scene was being represented using a slow frame-rate).
This implies a 'frame' paradigm, rather than a
continuous-motion paradigm (which in effect, implies a synchronous
versus asynchronous motion mechanism, which requires some sort of pulse
or clockline to keep things matched up.
Anyway, just thought I'd throw this your way to let you
know what kinds of things eidetic imagery tests can be used for in a
scientific framework (and, of course, for entertainment purposes).
I've had some quite intersting video games in my head played out,
so much more lucid than anything on playstation 2 or pcs.
You can contact this individual at [email protected].
AN IN-DEPTH LOOK AT DXM ABUSE
 A SCIENTIFIC LOOK AT THE GROWING PHENOMENON OF DXM ABUSE AMONG ADOLESCENTS
A SCIENTIFIC LOOK AT THE GROWING PHENOMENON OF DXM ABUSE AMONG ADOLESCENTS
by gravol
We are seeing an increasing number of news reports lately regarding
the abuse of DXM, and one DXM-containing medication in particular,
Coricidin Cough & Cold. Below, I have compiled abstracts from
medical papers that have been reported involving this abuse. With all
the attention DXM is getting in the media these days, it is interesting
to see the perspective that the Scientific community holds.
The Statistics of Coricidin Abuse:
This is brought to us via the University of California, San Francisco,
California Poison Control System, San Francisco Division, USA, in an
article by S. Banerji and I.B. Anderson. Cases involving ingestion of a
dextromethorphan-containing product recorded at a poison control center
were studied. A retrospective review of all consultations involving the
ingestion of Coricidin HBP Cough & Cold tablets recorded by the
California Poison Control System was conducted for the period from
January 1 to October 1, 2000. Computerized charts on the consultations
were reviewed to obtain data on patient age and sex, number of tablets
taken, reason for tablet ingestion, symptoms, treatment, disposition,
and outcome. A total of 92 charts (for 92 patients) documenting
Coricidin HBP Cough & Cold tablet ingestion were reviewed. The
reason for tablet ingestion was classified as abuse in 65 patients
(71%), a suicide attempt in 8 (9%), misuse in 1 (1%), malicious
administration in 1 (1%), and normal use (but with an adverse drug
reaction) in 1 (1%); 16 patients (17%) consumed the tablets for an
unknown reason. The 92 patients comprised 42 males and 50 females. Among
all patients, 78 (85%) were 13-17 years old, and among those classified
as having abusive intent, 58 (89%) were in the same age range. The most
commonly reported signs and symptoms associated with ingestion were
tachycardia (50 patients), hypertension (29), lethargy (40), mydriasis
(20), agitation (15), ataxia or dizziness (20), and vomiting (9).
Sixty-one patients (66%) had some alteration in mental status. Fifty-six
(61%) were treated in the emergency department; 11 (12%) were admitted.
All patients recovered completely. Information on the ingestion of
Coricidin HBP Cough & Cold tablets recorded at a poison control
center indicated a high rate of abuse of the product among teenagers.
Abuse Potential of Morphine/DXM medications:
This is brought to us via the Clinical Studies/Center for Chemical
Dependence, Johns Hopkins Bayview Medical Center, Baltimore, Maryland,
USA in a report by D.R. Jasinski. The potentiation of morphine analgesia
by dextromethorphan raises the issue of whether dextromethorphan also
potentiates those actions of morphine that lead to abuse. Clinical
pharmacology experiments indicated that dextromethorphan does not
potentiate the euphorigenic and miotic actions of morphine. Morphine
suppresses the dysphoric action of dextromethorphan. A second set of
experiments indicated that dextromethorphan does not alter the response
to naloxone-precipitated withdrawal. In a third set of experiments,
dextromethorphan did not alter the morphine-induced depression in the
slope of the increase in minute volume in response to breathing
increased CO2. In contrast to potentiation of analgesia,
dextromethorphan does not enhance the euphorigenic, physical dependence,
and respiratory depressant actions of morphine. These findings indicate
that dextromethorphan does not enhance the abuse potential of morphine
and that the potentiation of analgesia appeared to be selective.
DXM and Diphenhydramine/Ephedrine Abuse:
This comes via the Department of Psychiatry and Behavioral Sciences,
University of Oklahoma Health Sciences Center, Oklahoma City 73190-3000,
USA ( [email protected]
) by D.V. Gauvin et al. Two groups of rats were trained in a
two-choice drug discrimination procedure under a fixed-ratio 10 schedule
of food reinforcement. One group of rats (n=12) was trained to
discriminate the presence and absence of a drug mixture containing 10
mg/kg dextromethorphan + 10 mg/kg diphenhydramine. The other group of
rats (n=12) was trained to discriminate the presence and absence of
another drug mixture containing 10 mg/kg dextromethorphan + 10 mg/kg
ephedrine. Cross-generalization tests conducted with each of the
stimulus elements demonstrated that (1) the drug mixtures were not
perceived as new entities distinct from their component elements and (2)
the stimulus element saliency may be a factor determining the nature of
discriminative control by drug mixtures. Cross-generalization tests
conducted with the psychomotor stimulants, cocaine and amphetamine,
engendered complete generalization to the training cues in both groups,
whereas, pentobarbital engendered predominantly saline- or default-lever
responding. These data suggest a potential abuse liability for both of
these common over-the-counter drug mixtures and cautions against the use
of such combinations in pediatric patients.
Bulimia and DXM Abuse:
This comes to us via the Department of Pediatrics, Medical University
of South Carolina, Charleston 29425, USA in a report by L.D. Marsh et al
( [email protected]
). The comorbidity of bulimia and substance abuse is significant. The
substance that is abused may vary and the abuse potential for nonillicit
substances may be overlooked. This paper presents the first case
reported of dextromethorphan abuse and bulimia. It demonstrates the
complexity of assessment and treatment of bulimia and substance abuse of
over-the-counter medications.
Cough Syrup Abuse:
This comes to us via the School of Natural and Social Sciences,
Shepherd College, Shepherdstown, WV 25443, USA in a report by M.N.
Darboe. Drug abuse has been a national social problem in the United
States for decades and is often complicated by the emergence of new
types of abused drugs or new forms of abuse. The forms of abuse,
particularly by young persons, include the search for substitutes for
better-known substances. It is unclear, however, what factors determine
the choice of drug or substance for experimentation, considering the
wide range of choices. This paper attempts to delineate the factors
which make Dextromethorphan-based cough syrup an attractive choice.
Largest DXM Dose Ever Reported:
This comes to us via the Division of Emergency Medicine, University of
Utah School of Medicine, Salt Lake City in a report by T.R. Wolfe and
E.M. Caravati. The case of a 23-year-old man who was acutely intoxicated
on dextromethorphan and who was chronically addicted to the drug is
described. He consumed the highest daily dose for the longest duration
yet reported in the world's English-language medical literature.
Toxicity, abuse potential, and therapy of dextromethorphan intoxication
are discussed. Unfortunately, we do not have access to the entire
article and cannot disclose the actual amount that was ingested.
Cognitive Deterioration from DXM Abuse:
This comes to us via the University of Western Ontario, London, in a
report by A. Hinsberger et al. Dextromethorphan (DM), the dextrorotatory
isomer of 3-hydroxy-N-methylmorphinan, is the main ingredient in a
number of widely available, over-the-counter antitussives. Initial
studies (Bornstein 1968) showed that it possessed no respiratory
suppressant effects and no addiction liability. Subsequently, however,
several articles reporting abuse of this drug have appeared in the
literature. The drug is known to cause a variety of acute toxic effects,
ranging from nausea, restlessness, insomnia, ataxia, slurred speech and
nystagmus to mood changes, perceptual alterations, inattention,
disorientation and aggressive behavior (Rammer et al 1988; Katona and
Watson 1986; Isbell and Fraser 1953; Devlin et al 1985; McCarthy 1971;
Dodds and Revai 1967; Degkwitz 1964; Hildebrand et al 1989). There have
also been two reported fatalities from DM overdoses (Fleming 1986).
However, there are no reports describing the effects of chronic abuse.
This report describes a case of cognitive deterioration resulting from
prolonged use of DM. Again, we do not have access to the article and
cannot publish it in its entirety.
Teenage DXM Abuse:
Finally, this report is by S. Murray and T. Brewerton.
Dextromethorphan, the d-isomer of the opiate agonist levorphanol, has
none of the analgesic or sedative effects associated with the opiates
and is approved for over-the-counter use as an antitussive. It is
available, in various combinations with other medications, in
nonprescription cough suppressant and common cold formulations, and its
availability in the United States is not controlled. In this paper we
have reported two cases of recreational use of
dextromethorphan-containing cough syrup by two unrelated teenage boys.
Despite the safety of this medication when used at the recommended
dosage, there have been cases of "recreational" use of dextromethorphan
as well as death by overdose. Although usually thought to be
nonaddictive, dextromethorphan produces a substance dependence syndrome,
and physicians should be aware of its abuse potential, particularly by
youths.
TALES FROM THE DARKSIDE
 AND OTHER MACABRE TALES OF STRANGE BEHAVIOR BY DXM USERS
AND OTHER MACABRE TALES OF STRANGE BEHAVIOR BY DXM USERS
compiled by gravol
The following will be a monthly section that appears in the Zine
highlighting some of the strange behaviors of DXM users. This is not to
poke fun at the drug or the users, but to give you a little taste of
"shock therapy" so-to-speak. While some of the reports are rather
incredible, it is not advisable that you follow any advice given in this
section. It is simply meant for entertainment purposes only. In fact,
most of the stuff reported here is downright disturbing...
DXM Enema:
The first case comes to us from a male named "BRO." He claims: "
I did the DXM enema a few weeks ago and I definately don't recommend
it, but put it to the test if you want to. It may work well for you. I
did it pretty much the same way it is recommended on the Third Plateau.
[Editor's Note: The Third Plateau is a DXM community website, located at http://www.third-plateau.org ]
It was real uncomfortable. It burned and filled my lower intestine
with lots of pressure and gas. I was forced to shit it out then I just
swallowed a pill. I would rather just go through the nausea and throwing
up which is caused through taking it the good ole fashion way. The
nausea doesn't last that long anyways and the throwing up kinda feels
good after its over."
Bottom line is this, folks... if you don't like the taste of
something, that is no need for you to shove it up your.... well, you
know what. In fact, there are reportedly a few individuals who are doing
this practice. Maybe we should call Ripley's Believe-it-or-Not?
A Dog on DXM:
One DXM user was so bored he decided to feed 214mg of DXM to his dog,
named Zeus. The user, whose identity we have concealed, states
"If you're planning on dexing your dog, here's how I managed to do it.
Cap some powder, or put it in an olive, whatever. I ended up wrapping
my powder and whatever was left of the first capsule i tried giving it
in an apple skin, then, basically shoved it down his throat. lol
He tore my hand apart but, seeing my dog do the Robo-shuffle was worth
the trouble."
Very, very disturbing. We are happy to note, however, that the dog is apparently fine.
Penis Shrinkage:
One DXM user, VanillaDEX, reports a rumor he heard from a friend that
if you use DXM more than 3 times a month your penis will shrink. The
totaly absurdity of this rumor makes it rather entertaining, but similar
rumors have been started about LSD and have been carried to great
lengths by paranoid trippers. We are happy to report (at least from the
perspective of yours truly, the Editor) that no such thing exists. In
fact, low doses of DXM and afterglow can cause a prolonged erection and
make the females quite happy. So I guess DXM might be an alternative to
that Stay-Hard cream.
 Psych Ward:
Psych Ward:
And lastly, whatever you do, do not take advice from this individual, who goes by the handle cykros:
"just over two weeks ago i decided to get a bottle and a half (12 oz,
1064 mg) of tussin, and downed that, expecting a really nice 4p trip,
with a pot of coffee waiting if i got sleepy...anyway, i stayed online
too long, and my dad found me all bugged out at the computer not even
knowing where i was....really bad shit, not that it was a bad trip, just
had bad results. Anyway, i ended up in the hospital that nite
(btw, had an awesome OOBE, only upside )and stayed in the icu
before going to my own room...later found out i was labeled suicidal,
homicidal (due to threats made while tripping), and impulsive, which got
me thrown into yale psychiatric hospital for the last fucking two
weeks....sucked major donkey balls, word to the wise, don't get fucking
caught . Anyway, i'm tripping now (hehe, got out earlier
today, didn't waste much time...) so i guess i'll wrap this up...i just
wanted to allow others to learn from my stupidity."
Well, that is all for this issue. We will try to get these individuals
some psychiatric care and in the meantime, look forward to more
tantalizing tales of the just plain weird.
DXM ARTWORK
A COMPILATION OF ARTWORK DONE UNDER THE INFLUENCE OF DXM
compiled by gravol
Below is several pieces I did while under the influence of 2nd plateau
trips. The first one is a colored pencil drawing of Notre Dame
Cathedral in France. The other three I did in regular graphite pencil.
The last one was the most difficult, and it took several weeks to
complete. You can view the drawing in its entirety on the web at http://www.lesia.org/amiens.jpg


Notre Dame Cathedral
Jack
Nicholson
A
Metamorphosis
Paris,
France
The Shining A Dove in a Hand
 Amiens Cathedral, Paris, France (Full picture at http://www.lesia.org/amiens.jpg )
Amiens Cathedral, Paris, France (Full picture at http://www.lesia.org/amiens.jpg )
OTHER ARTWORK
by various artists
The following pieces come courtesy of the Third Plateau Website, which
is highly based in the arts. If you would like a piece submitted,
please contact the Editor at [email protected].




Painting by
Computer- Drawing
by Grrinded
Self-portrait by
Mad Hatter Painting
by
NHaedhroes in
DextroMeth pastel
Finally, in the Artists Spotlight Section, we have two paintings by
murmurmaid from the Dextroverse Community. Keep up the good work!!
Submit your artwork to win a chance at free DXM!


INFO ON ORDERING PURE DXM POWDER
compiled by gravol
There are only two reliable sources for obtaining dextromethorphan
powder for research purposes. One is Chico Chemical and the other is LTK
Research Products. Neither of these companies are affiliated with the
Zine. Information, taken from their website, follows.
If you are a company that sells DXM powder and would like
to be noted in this section, please contact the Editor. Unfortunately,
we've had many cases of fraud in the past years so we're only posting
the most credible sources.
Chico Chemical
Chico Chemical is a chemical reseller based in Winston-Salem, NC
-offering fine chemicals and bulk actives with a market focus on small
research entities that require special attention and personalized
service. We purchase only the finest quality product in bulk enabling
smaller customers to get the product they need at an affordable price.
Our
inventory is growing, and options for payment are being added everyday
so feel free to email us about how we can be of service to you.
Mail: 353 Jonestown Rd. - Suite 169 - Winston-Salem - NC - 27104
Email: [email protected]
25 grams $45
50 grams $79
100 grams $139
* $5.00 S&H on all
orders
Most orders will ship within 48 hours.
Avg. Delivery Time 2-3 Days in the USA
The U.S. Department of Health and Human Services Food and Drug
Administration regulates the sale and use of these chemicals. Chemicals
are sold only for use as approved by the FDA. The use of these chemicals
may be further limited or regulated by federal, state, or local
government. Buyer is responsible for compliance to applicable laws and
regulations. Buyer expressly warrants that they will use chemicals
purchased in accordance with all applicable laws and
ordinances.
1. Delivery
All sales are FCA Seller's shipping point. Seller's delivery to the
carrier constitutes delivery to Buyer and Buyer assumes all risk of loss
or damage during transit. The purchase price of all products includes
shipping via United States Postal Service Priority Mail, however, Seller
reserves the right, in it's discretion, to determine the method of
shipment. Upon receipt of all goods, Buyer must immediately inspect the
material and make a claim to Seller in writing for all shortages or
defects. All claims must be made to Seller within five days of
receipt by Buyer. If no claims are made within the five days, it will
bedeemed that the goods conform to these terms of sale, and have been
irrevocably accepted by the Buyer. If Seller
determines that the products named in Buyer's claim are defective,
inadequate, or otherwise incorrect, the Buyer is eligible for a
full refund of purchase price or a replacement of the product. Buyer
must return products to Seller in the accordance with Seller's
instructions.
2. Warranties
Seller warrants that its products shall conform to the description of
such products as provided to Buyer by Seller through Seller's catalog or
other literature. THIS WARRANTY IS EXCLUSIVE, AND SELLER MAKES NO OTHER
WARRANTY, EXPRESS OR IMPLIED, INCLUDING ANY IMPLIED WARRANTY OF
MERCHANTABILITY OR FITNESS FOR ANY PARTICULAR PURPOSE. Warranty is
ineffective if Seller determines that Buyer has misused the
products in any way, has failed to use the product in accordance with
industry standards, or has failed to comply with any applicable
regulations regarding the use of the material.
3. Buyer's Use of Products
The U.S. Department of Health and Human Services Food and Drug
Administration regulates the sale and use of these chemicals.
Chemicals are sold only for use as approved by the FDA. The use of
these chemicals may be further limited or regulated by federal,
state, or local government. Buyer is responsible for compliance to
applicable laws and regulations. Buyer expressly warrants that they
will use chemicals purchased in accordance with all applicable laws and
ordinances.
To order by mail with a check or money-order:
1. Print, sign and date a copy of the Terms of Sale Agreement.
2. Print and fill out an Order Form.
3. Photocopy your valid state ID or drivers license. **
4. Mail the signed Terms of Sale, Order Form, and the copy of your ID
along with a certified check or money order for the amount of order
(made payable to Chico Chemical) to:
353 Jonestown Rd - Suite 169 - Winston-Salem - NC - 27104
* There is a $10 S&H fee for mail orders.
** ID needed for age verification only. Name on ID should match
signature on Terms of Sale Agreement.
LTK Research Products
LTK Research Products is a research chemical company located in Minot,
North Dakota . We currently offer Quality research chemicals at a
low competitive price. We are now offering our products over the web as
well as by mail
If would like to contact us you can:
by mail: LTK Research Products
2001 8 th Ave SE Suite F
Minot, ND 58701
by Phone: 1-866-LTK-PROD/1-866-585-7763 between 10am and 4pm cst
by Fax: 1-701-839-0891
by e-mail: [email protected]
Orders by Check or Money orders: If the web page ordering system does
not fit your needs you can order anything from this site by Mail.
Please send your order to :
LTK Research Products LLC
2001 8 th Ave SE Suite F
Minot, North Dakota 58701
Please include the following :
- A return address
- Enclose a check or money order
- Make payable to:
LTK Research Products
- Include a $15.00 fee for shipping and handling
- There is a $9.00 added charge for express deliveries
- Name of chemical(s) you want
- Amount(s) of chemical(s)
- Photo copy of ID on all orders over $500
- We do not deliver to P.O boxes
- An e-mail address would be helpful to let you know
- If there are any problems
- No COD
Shipping: Paypal Shipping Rates: $50.00 - $99.99
$15.00 Priority mail/Delivery confirmation
$100.00 - $199.99 $20.00 Same as above
$200.00 - and over $30.00 Express Mail delivery
If you need overnight delivery you will have to call for a price
quote. We send overnight deliveries via Fed Ex or Airborne Express. We
will only ship to a confirmed address. If you place an international
order you may be subject to additional fees and verification before you
order is sent.
Credit Cards orders by phone: coming soon
30 grams.....$ 65.00
50 grams....$ 125.00
100 grams...$ 197.00
* If you are interested in a bulk price quote for Dextromethorphan
Hydrobromide please e-mail for price and availiblity
Dextromethorphan Hydrobromide
U.S.P.,
N.F., F.C.C Grade, 99.5+%
C
H NO - Hbr
F.W. 370.33
18
25
LTK Research Products LLC does not warrant that products supplied by
LTK Research Products LLC are listed in Toxic Substances Control Act
inventory list. The purchaser assures the use of the product/s
purchased from LTK Research Products LLC will be in full compliance with
the TSCA and its regulations.
Orders by Check or Money orders: If the web page ordering system does
not fit your needs you can order anything from this site by
Mail Please send your order to :
LTK Research Products LLC
2001 8 th Ave SE Suite F
Minot, North Dakota 58701
LTK Research Products is in the process of creating a web page to
direct researchers to interesting and exciting developments occuring
with our products. At LTK Research Products, we provide you with the finest research products available.
Dextromethorphan Hydrobromide-USP Grade
This chemical is currently used in investigations for preemptive use on postoperative analgesic requirements.
See Sanoa A. K.Helmy, MD, Ayham Balij, MD; Anesth Amalg 2001;
92:739-744
*All Refunds / Credits will be Issued within three business days
upon receipt of the returned product.
Execptions: Due to the nature of our products we cannot accept
returned products that have been opened. If you have a problem
please contact us right away, so we can work quickly to resolve
your problem. All returns will be subject to a $10.00 restocking
fee.
Our Goal @ LTK Research Products is 100% Customer SatisfactionIf
for any reason you are unsatisfied please contact us @ 1-866-
ltk-prod or 1-866-585-7763
ACKNOWLEDGEMENTS
I wish to thank everyone who either contributed to the Zine or helped
provide information on DXM. I would especially like to thank void and
Vaesolis from the Dextroverse and all the helpful people from that site
and others that helped me compile this massive publication.
Next Issue: Vaesolis Meditation Technique Update, and Much Much More!
Also, don't forget to look for the 5-year Anniversary Special in
December!

About the Editor:
Gravol, also known as Jeff, is 24 and works on the Zine in his spare
time. Born in Phoenix and having lived in Akron, Ohio, for
several years, he now resides in St. Augustine, Florida. He is also
the author of the Dramamine FAQ, found at lycaeum.org, and an artist in
his spare time. To check out some of his work, goto http://www.lesia.org/amiens.jpg. You can find him posting at Usenet's alt.drugs.psychdelics, as he is a regular there.
* If you'd like to contribute an article or any information to the DXM Zine, email [email protected]. The Zine is free, but any contributions
reduce the tremendous amount of time it takes to complete it would be
helpful in maintaining its free distribution. Thank you!

{kind=link}